September 2017- Our experience with these patients highlights that ENKTCL does indeed occur in SSA, increases familiarity with ENKTCL among clinicians and pathologists throughout the region, and emphasizes the need for better diagnosis and treatment for this neglected population.
Extranodal natural killer/T-cell lymphoma in Malawi: a report of three cases
Tomoka, T, Powers, E, van der Gronde, T, Amuquandoh, A, Dhungel, B. M, Kampani, C, Gopal, S
BMC Cancer
Access the full article here.
Background
Extranodal NK/T-cell lymphoma (ENKTCL) reports from sub-Saharan Africa (SSA) are remarkably rare, despite early childhood acquisition and high prevalence of the causative infectious agent, Epstein-Barr virus (EBV), and frequent occurrence of other lymphoproliferative disorders causally associated with EBV.
Case Presentations
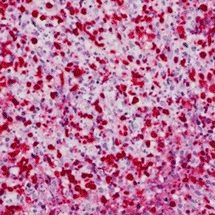
At a national teaching hospital in Malawi, three patients of African descent were seen with ENKTCL between 2013 and 2014. Patients were aged between 29 and 60 years, two with craniofacial involvement and one with a primary abdominal tumor, and all were HIV-negative. All had systemic B symptoms, and two severely impaired performance status. On histologic review, morphology and immunophenotyping demonstrated classical ENKTCL features in all cases, including diffuse proliferations of intermediate-to-large atypical lymphocytes with high mitotic activity and extensive background necrosis, positivity for CD3 and CD56, and negativity for CD20. By in situ hybridization, all three tumors were positive for EBV-encoded RNA (EBER). Baseline plasma EBV DNA was also markedly elevated for all three patients. Due to radiotherapy and chemotherapy limitations, patients were treated with CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) with rapid disease progression. All three patients died from progressive lymphoma within 3 months of initial diagnosis.
Conclusions
Our experience with these three patients in Malawi can highlight that ENKTCL does indeed occur in SSA, increase familiarity with ENKTCL among clinicians and pathologists throughout the region, and emphasize the need for better diagnosis and treatment for this neglected population.