July 2016 – To make early detection of breast cancer in Malawi possible, training laywomen to screen seems to be a viable option. 1000 examinations provide the evidence that the quality of these screening compares to screenings performed by clinicians.
Clinical breast exam screening by trained laywomen in Malawi integrated with other health services.
Gutnik L, Lee C, Msosa V, Moses A, Stanley C, Mzumara S, Liomba NG, Gopal S.
Journal of Surgical Research
Full text available at PubMed and Journal of Surgical Research.
Abstract
Background
Breast cancer awareness and early detection are limited in sub-Saharan Africa. Resource limitations make screening mammography or clinical breast examination (CBE) by physicians or nurses impractical in many settings. We aimed to assess feasibility and performance of CBE by laywomen in urban health clinics in Malawi.
Methods
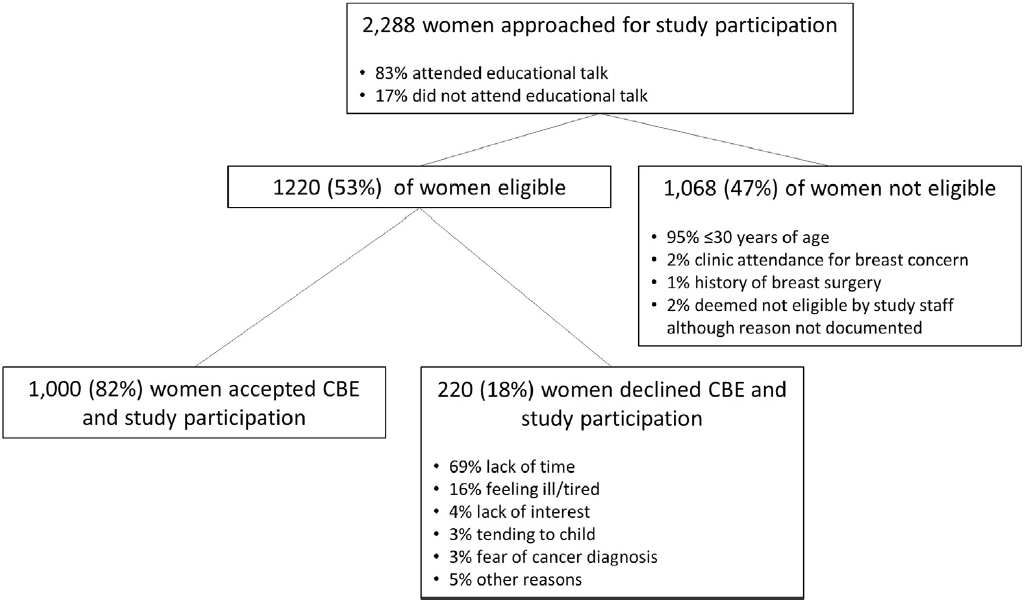
Four laywomen were trained to deliver breast cancer educational talks and conduct CBE. After training, screening was implemented in diverse urban health clinics. Eligible women were ≥30 y, with no prior breast cancer or breast surgery, and clinic attendance for reasons other than a breast concern. Women with abnormal CBE were referred to a study surgeon. All palpable masses confirmed by surgeon examination were pathologically sampled. Patients with abnormal screening CBE but normal surgeon examination underwent breast ultrasound confirmation. In addition, 50 randomly selected women with normal screening CBE underwent breast ultrasound, and 45 different women with normal CBE were randomly assigned to surgeon examination.
Results
Among 1220 eligible women, 1000 (82%) agreed to CBE. Lack of time (69%) was the commonest reason for refusal. Educational talk attendance was associated with higher CBE participation (83% versus 77%, P = 0.012). Among 1000 women screened, 7% had abnormal CBE. Of 45 women with normal CBE randomized to physician examination, 43 had normal examinations and two had axillary lymphadenopathy not detected by CBE. Sixty of 67 women (90%) with abnormal CBE attended the referral visit. Of these, 29 (48%) had concordant abnormal physician examination. Thirty-one women (52%) had discordant normal physician examination, all of whom also had normal breast ultrasounds. Compared with physician examination, sensitivity for CBE by laywomen was 94% (confidence interval [CI] 79%-99%), specificity 58% (CI, 46%-70%), positive predictive value 48% (CI, 35%-62%), and negative predictive value 96% (CI, 85%-100%). Of 13 women who underwent recommended pathologic sampling of a breast lesion, two had cytologic dysplasia and all others benign results.
Conclusions
CBE uptake in Lilongwe clinics was high. CBE by laywomen compared favorably with physician examination and follow-up was good. Our intervention can serve as a model for wider implementation. Performance in rural areas, effects on cancer stage and mortality, and cost effectiveness require evaluation.