Almost 40 years after the discovery of HIV, a new NOVA program “Ending HIV in America” reflects on the history of one of the most elusive and deadly viruses to ever infect humans. Dr. Myron “Mike” Cohen, director of the UNC Institute for Global Health & Infectious Diseases is the architect and principal investigator of the multinational HIV Prevention Trials Network (HPTN) 052 study that demonstrated antiretroviral treatment prevents the sexual transmission of HIV-1, recognized as the “Breakthrough of the Year” in 2011. Dr. Cohen was interviewed for the NOVA program that premiered Oct 5 on PBS and following is the extended interview.
How do you approach infectious disease research?
“The most important thing about any infection is to understand the rules, and COVID is a good example. We needed to understand the rules that govern transmission of the infection and we spent a lot of time trying to understand the rules that govern the transmission of HIV. We learned about the kinds of behaviors and exposures that allowed transmission of HIV and with what efficiency. For example, in the very beginning of the epidemic, getting a unit of contaminated blood was nearly 100% infectious. Blood banks needed to protect the blood supply. We learned needle sticks could transmit HIV. We learned that sexual transmission was possible, and that the probability of a transmission was governed by the concentration of virus in the infected person. We came to understand which people living with HIV had more virus and who had less, and why. We learned that some behaviors were riskier than other behaviors.”
Once you understood the rules, what were the obligations?
Credit: Smithsonian Institute
“We needed to prevent HIV, we needed to treat HIV, and we needed to cure HIV. My research team was committed to prevention of HIV in the absence of a vaccine, and that required different activities. One activity was “non-pharmacologic” intervention. We worked very hard to inspire behavior changes that included safer sex and using condoms. We came to understand through this work, that other sexually transmitted infections (STIs), especially some of the bacterial and viral diseases, like gonorrhea and herpes, could amplify the transmission of HIV by increasing the concentration of virus in the genital tract of the person who has HIV and such STIs, causing, inflammation or ulcers, in people who did not have the infection. This greatly increased susceptibility to infection.
“Of course, we were constantly looking for biomedical tools to stop the spread of HIV. Our earliest work showed that treatment of STIs decreased the concentration of HIV in the genital tract. But several large mass population treatment trials showed that treating STIs, while important in and of itself, could not stop the spread of HIV.
“As soon as antiviral drugs directed at HIV became available in 1989, our group began to work on their use beyond treatment, for HIV prevention. The idea was, let’s use antivirals to stop the spread of HIV. There were two options: 1) As we treat people with HIV infection to stop the progression of infection, to what extent will we render them no longer contagious? 2) And then, what about HIV negative people at risk for HIV exposure. Could we use antivirals as pre-exposure prophylaxis? We knew there had been success in pre-exposure prophylaxis in other diseases. For example, if you’re planning to go to a malaria infested area, you can take medication to prevent infection. We created many mathematical models of these approaches focusing on antiviral therapy for treatment as prevention. And we began laboratory and animal experiments to explore these hypotheses.”
How did you get involved with HIV infection?
UNC began treating blood disorders in 1947, starting with Kenneth Brinkhous (right) who studied the first known canine carriers of hemophilia. This led to the the creation of the Francis Owen Blood Research Laboratory, which set the stage for major breakthroughs in hemophilia and HIV. (photo courtesy of the Francis Owen Blood Research Laboratory)
“My wife, Dr. Gail Henderson, and I had been working in China and came back to the US, both getting jobs at UNC. The constellation of symptoms that constituted AIDS had just been described in late 1980 as we arrived. In Chapel Hill, we had a large number of people living with hemophilia. Dr. Kenneth Brinkhaus and other scientists at UNC had developed treatments for hemophilia using infusions of plasma blood clotting factors. I was asked to consult on a young man with hemophilia who had fever and swollen glands. I examined him and thought to myself, this gentleman has AIDS. At that time, it was a terrific concern that the blood supply had been contaminated with whatever agent was causing AIDS. But we didn’t know what the agent was. Because of UNC’s pioneering hemophilia research including the Francis Owen Blood Research Laboratory, we had thousands of people with hemophilia living in the North Carolina. As a result, AIDS very quickly became a common infection at UNC. By 1984, perhaps 15% of UNC hospital admissions were for management of AIDS. During any major outbreak or disease epidemic, an all-hands-on deck approach is needed. At that time there were only a small number of infectious disease specialists, and we all became involved in the management of AIDS.”
Why was it affecting hemophiliacs?
“Hemophiliacs would occasionally have bleeding from minor trauma that could be stopped by infusion of blood clotting factors. AIDS first surfaced in men who have sex with men, so some time went by before we learned blood and blood products were contaminated with a transmissible agent. HIV had not been discovered and no one knew what the transmissible agent might be, or how to get rid of it. And so, during the window of time between recognition of AIDS and the discovery of HIV, these contaminated blood products worldwide constituted a tragedy for anyone who required blood products. Once HIV was discovered, tests were developed to detect it, and strategies were emergently developed to eliminate HIV from blood products.”
Can you give us a brief history of AIDS from when you first encountered it?
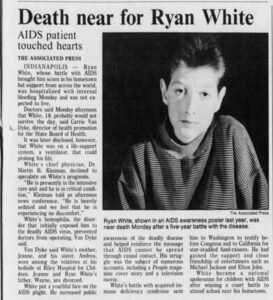
Ryan White was 13 when he was diagnosed with AIDS after a blood transfusion in December 1984. Credit: Associated Press
“By 1985, many patients were admitted to UNC Hospitals (then North Carolina Memorial Hospital) for management of AIDS. We needed to rapidly expand the number of health care providers who could take care of people with this infection and provide the best care we could in the absence of drugs to stop the replication of the virus. Basically, we treated opportunistic infections and cancers that arose as AIDS progressed. The Triangle was a special place because we had Burroughs Wellcome (now GSK) team, our friends and neighbors, who developed the remarkable drug AZT. It is hard to describe the moment when we realized that this drug could stop the replication of HIV. But it quickly became apparent the virus could acquire resistance to any one drug, and so other drugs were developed. The development of drugs to treat and prevent HIV infection continues to this day.
“At first, a large combination of individual drugs was used, which was pretty cumbersome because you had to take a lot of pills a day (referred to as a pill burden). It wasn’t until 2006 that we got to one pill a day. So, this is a very long story as it relates to putting combinations of drugs into a single pill. UNC investigators including Drs. Stanley Lemon, Margaret Smiley, Charlie van der Horst, Joe Eron, David Wohl, Angela Kashuba, Ron Swanstrom, Ada Adimora, David Margolis and many, many others, played a major role in the development of drugs to treat HIV.”
When did you first have the idea of antiretroviral drugs for prevention of HIV and AIDS?
“I had been working on sexually transmitted diseases, particularly, gonorrhea, to understand how the disease was transmitted from one person to another. As I was drawn more and more into the HIV field, the same thinking applied. By the late 1980s, my research group was studying the transmission of HIV.
“In 1989, I went to a Burroughs Wellcome event to celebrate the success of AZT before the announcement of the clinical trial results. The late Dr. David Barry, who directed the company’s AIDS research, shared the trial results with in me in detail. It was at that moment that I asked the question. ‘Can we work with you on this drug to understand if we can stop the transmission of HIV?’ That night was the beginning of the rest of my next 30 years of work.”
When you first thought of the idea, was it just AZT?
Credit: National Museum of American History
“My collaborators, Angela Kashuba, Ron Swanstrom, Susan Fiscus, Rick Tidwell and a big team of students and postdoctoral fellows studied the effects of AZT, our only antiretroviral drug at the time, on the transmission of HIV. We were particularly concerned about where AZT went in the body when taken as a pill. Did it actually get into the genital secretions of men and women where it might kill the virus? And how was it metabolized? We pursued as many details of AZT biology and pharmacology as possible.
“And as other drugs were developed, we’d look at the biology of each agent. With NIH support we were committed to determining how much virus was in the male and female genital secretions, which we believed governed HIV transmission, and the effects of the antiretroviral drugs on replication of HIV in the genital tract. Importantly, this work led to the hypothesis that antiretroviral drugs could stop the transmission of HIV. But we concluded that only a large randomized clinical trial could demonstrate the actual benefits of “treatment as prevention” and antiretroviral drugs as pre-exposure prophylaxis.”
What would you say were the barriers to starting a clinical trial for “treatment as prevention?”
“First, the treatment community was rightly most concerned about creating the best quality of life for HIV infected people. Antiretroviral drugs saved people’s lives. The potential public health benefits were less compelling to the treatment community. Second, I think most experts believed the “treatment as prevention” idea had merit, but it just did not attract enough momentum to get a huge wave behind it. Most experts believed the trial design required to understand “treatment as prevention” was way too hard, ethically challenging, and perhaps too complex to be successful. But in all candor, our group at UNC, and our partners at the NIH, HIV Prevention Trials Network and Family Health International (now FHI360), were tenacious and very committed to the idea. So, we just kept going.
“A giant barrier to a treatment as prevention trial was the ability to secure enough drugs to conduct the trial, and to provide HIV infected people continued treatment when the trial ended. We went iteratively to each manufacturer to ask for help. This was a request for exceptional philanthropy, because the drugs were valuable and precious. And in fact, it was our neighbors at GSK that got the trial off the ground. They were making a drug called Combivir, which was a powerful and popular combination drug that included AZT. They donated a huge amount of the drug for the prevention trial. I can’t say enough about their support. And then five or six other companies came on board. When the last company agreed to support the trial, I sent two dozen roses to the physician who managed the company’s philanthropic supply. This was a huge moment in a decade long crusade toward proving “treatment as prevention.”
Would you say this was a true example of a public private partnership?
“This was the ultimate public private partnership. The work we were doing was under IND (FDA-Investigational New Drug), but not seeking licensure approval for this purpose. The trial we conducted was called HPTN 052; the trial started around 2007, and addressed the primary endpoint of the hypothesis–prevention of HIV transmission–in 2011. We enrolled “discordant” couples where one partner was HIV infected, and the other was HIV negative. We were asking two questions: If we give antiviral treatment to HIV infected people earlier than usually started can we prevent HIV transmission to the negative sexual partner, and can we demonstrate that earlier treatment benefits the health of the person with infection?
“The results were presented at the International AIDS Society in Rome in July 2011, to an audience of about 10,000 people. The meeting organizers provided an hour for the presentation and stopped all other activities. The results–that we could durably stop transmission of HIV through treatment–were met with remarkable enthusiasm, to say the least.”
How did the discovery rapidly change patient care?
“When we realized that we’d stopped the transmission of HIV by treating the infected person, the immediate, overnight question became why are we rationing these drugs? People needed to be treated immediately. The realization that antiretroviral treatment not only saved your life if you were HIV infected, but would also stop onward transmission was ‘Why aren’t we finding everyone who is infected so that we can test and treat them?’ At this moment in time, management of HIV infection changed and the clinical trial HPTN 052 was recognized by Science Magazine as the science breakthrough of the year in 2011.”
What was the process for getting the results? Tell us about the oversight committee.
“When investigators choose to do a clinical trial, it has the greatest weight if the results are randomized and if possible blinded, so that there is no bias. In this particular trial, we had to develop an ethical way to compare treated and untreated people. We were managing both couples and individuals, and we knew that we would ultimately treat everyone HIV infected in the trial. An oversight committee called the Data Safety Monitoring Board (DSMB) met routinely to oversee blinded results, prospectively. They could see results as they were accruing. They met to make sure the trial was safe because the DSMB is empowered to stop any research trial for a variety of reasons, including safety, success and/or failure. We enrolled more than 1,300 couples in 11 countries, and we met with our oversight committee every six months.”
How did you go from meeting with the DSMB every 6 months to achieving success?
“We were working hard on the study but because the study was blinded, we had no idea what was happening with the results from 2007-2011. As the leader of the team, I would ask, somewhat tongue-in-cheek, for the results at every meeting with the oversight board, and they would say no. But then at the 11th meeting in spring 2011, the team went in and I sat down. But then they told me to stand up. As always, I asked the oversight board if they could tell us something. On this occasion, they acknowledged that they did have a recommendation but said “we can only tell the NIH, the sponsor of the study, our recommendation.”
Campus of the National Institutes of Health in Bethesda, Maryland.
“We left this meeting shocked. We thought the study had failed. One of my colleagues, who was supposed to drive me to the airport was so upset that I told her to take me to the Metro instead. I planned to return to Chapel Hill and wait for more news. But it was just as I was getting out of the car at the Metro stop that I got a phone call from the NIH who asked the team to come back to the campus. So, we all drove over to the NIH and went into a conference room with a large group of people. Everyone associated with the HPTN 052 study from NIH was there. There was a huge stack of papers on the table and after a few minutes of mischievous equivocating, the Director of the NIAID Division of AIDS, Dr.Carl Dieffenbach, put his hands on the stack and said, “Congratulations, this is a home run!”
“We then were told that we had stopped the transmission of HIV from an infected person to their sexual partner through successful treatment. We also learned that earlier treatment benefited the health of the individual subjects. These results were ultimately reported in a series of papers in the New England Journal of Medicine and the Lancet.”
What were the concrete results for HIV patients?
“The history of HIV drug development is important. AZT was not without side effects, and it was believed that HIV treatment should be delayed. This also reflected the fact that drugs were not available in most resource constrained countries. At the time we learned the results of HPTN052, antiretroviral drugs were still rationed, although treatment was starting earlier and earlier in the course of the diseases. Once it was realized that you render people no longer contagious through treatment, everything changed. The strategy increasingly focused on treating when the disease is detected, making more drugs, and drastically increasing efforts at the earliest possible detection of infection.
“And so, treatment as prevention became the central strategy for HIV prevention. In all candor, the work we did might have been considered trivial if the benefit was only 30%, but at near 100% benefit, treatment as prevention became a gamechanger. Our work was mostly limited to heterosexual couples, but later work from England and Australia showed this idea works in men who have sex with men as well.”
Credit: Aidsmap
Can you describe your experience at the 2011 International AIDS Society in Italy?
“We had an hour to present the results of the study, and we’d rehearsed and planned for this moment for a decade. There were approximately 10,000 people at the meeting attending different sessions. People listened in overflow rooms as we presented irrefutable results that showed that successful treatment of HIV with antiretroviral drugs stopped the sexual transmission of HIV.
“When my colleagues and I finished our presentation, I sat down, and for a moment there was total and complete silence. Then, the conference erupted in applause with a massive and sustained standing ovation. I remained seated because I did not quite know what to do. It was really an emotional, remarkable moment, and anyone who was there will remember. People were so excited. Here was something that really worked and would change the management of HIV.”
“HPTN 052 is the foundation for all current strategies, the study and its findings have inspired the world to hope for an AIDS-free generation. It literally changed the path of HIV/AIDS and saved millions of lives and new infections. Public policy was turned upside down and WHO, CDC, NIH and HRSA released all new treatment guidelines. In fact, the U=U (HIV Viral Load and Transmissibility of HIV Infection) campaign was built on this research. As well as Dr. Anthony Fauci’s national plan announced in JAMA in March 2019 to “end the HIV epidemic in the U.S.”
What is something that you’re particularly excited about that you’re working on right now?
“There’s nothing we’re doing now that I don’t believe is important to the prevention of HIV. As a leader of the HIV Prevention Trials Network (HPTN) our results have implications worldwide. We have sites in Asia, Africa, Latin America and the United States. In 2021, NIH and HPTN, working with ViiV, received FDA approval for the ViiV drug Cabotegravir for the prevention of HIV in men and women. This is the first injectable long-acting pre-exposure prophylaxis drug, and it has generated much excitement. Studies in men in the Americas were directed by Dr. Landovitz at UCLA and studies in women in Africa were led by Dr. Delaney, younger colleagues I have had a chance to work with over the course of their careers.
“Working with our partner the HIV Vaccine Trials Network (HVTN) we recently reported the first monoclonal antibody (mAB) to prevent HIV infection. With my colleague in Seattle, Dr. Larry Corey (who I first met in 1977) I had the opportunity to play a leadership role in this very large multinational study.
“When COVID came along in 2020, I also got a chance to play a role in COVID Prevention and play a leadership role in the new NIH COVID Prevention Network (CoVPN), which fused the NIH HPTN and HVTN, and another group, the NIH Infectious Diseases Clinical Research Consortium. We worked on vaccines and monoclonal antibodies directed against SARS-CoV-2. The 40 years of work on HIV directly informed and inspired everything we did with COVID-19. The UNC Infectious Diseases team, including clinicians and scientists across our campus, worked together successfully on local interventions and with CoVPN. So, I believe, UNC played an outsized role in COVID prevention and treatment.”
What in your opinion is the last mile to overcome to end AIDS?
“We have two options: Find reliable and affordable ways to prevent HIV infection or cure the infection. Lifelong treatment leads to a healthy life, but curing the infection remains critical. Brilliant people worldwide are working on both of these goals. The only way to finish the last mile is to use an integrated set of strategies that deploy all our tools, like a puzzle that fits together. And in general, tight control of infectious diseases require safe, affordable, effective vaccines.”
How confident are you that the future generation of HIV researchers and scientists will carry on?
“I’m quite confident about the future HIV investigators. Consider how the vaccine field is progressing. Moderna has started clinical trials for an experimental HIV vaccine that uses the same kind of mRNA technology as in the COVID vaccine. We also see colleagues at Duke working on what’s called sequential vaccination. There is never a shortage of people who move to Chapel Hill (and Durham) who are passionate about fixing this problem. Their passion is compelling and inspiring.”
Can you prevent a novel virus like HIV or COVID from popping up in the future and affecting the world the way these have?
“We are of course always very concerned about public health and infectious diseases interventions. We humans live in a sea of microorganisms. I think the importance of my specialty, infectious diseases, is that this discipline lies in the interface between science and medicine and public health and public policy. It is certain that Sars-CoV-2 is not our last foe. Indeed, we’ve been dealing with Ebola Sudan, recurrence of polio, and Monkeypox. There will be more and more microbial challenges. The best we can do is learn from every experience and prepare better.”
What is the best that we can hope for to prepare ourselves, for pandemic preparedness or virus preparedness?
“It took us from 1980 to 1984, to identify HIV as the cause of AIDS, and from 1984 to 2011, to figure out a way to prevent HIV with treatment. On the other hand, It took two weeks to figure out the cause of COVID-19, two months to make a monoclonal antibodies mAbs, and 10 months to make mAbs and vaccines available. While scientific challenges facing us are vast, our abilities have proven amazing. Our experience with COVID-19 shows that policy and communications issues are just as important as biological solutions. This brings me back to the essential nature of integrated strategies in medicine and public health: behavioral scientists, social scientists and political scientists, among others, have a big role to play in helping us understand how to best protect public health in the 21st century.”
 Almost 40 years after the discovery of HIV, a new NOVA program “Ending HIV in America” reflects on the history of one of the most elusive and deadly viruses to ever infect humans. Dr. Myron “Mike” Cohen, director of the UNC Institute for Global Health & Infectious Diseases is the architect and principal investigator of the multinational HIV Prevention Trials Network (HPTN) 052 study that demonstrated antiretroviral treatment prevents the sexual transmission of HIV-1, recognized as the “Breakthrough of the Year” in 2011. Dr. Cohen was interviewed for the NOVA program that premiered Oct 5 on PBS and following is the extended interview.
Almost 40 years after the discovery of HIV, a new NOVA program “Ending HIV in America” reflects on the history of one of the most elusive and deadly viruses to ever infect humans. Dr. Myron “Mike” Cohen, director of the UNC Institute for Global Health & Infectious Diseases is the architect and principal investigator of the multinational HIV Prevention Trials Network (HPTN) 052 study that demonstrated antiretroviral treatment prevents the sexual transmission of HIV-1, recognized as the “Breakthrough of the Year” in 2011. Dr. Cohen was interviewed for the NOVA program that premiered Oct 5 on PBS and following is the extended interview. 


 “This was the ultimate public private partnership. The work we were doing was under IND (FDA-Investigational New Drug), but not seeking licensure approval for this purpose. The trial we conducted was called HPTN 052; the trial started around 2007, and addressed the primary endpoint of the hypothesis–prevention of HIV transmission–in 2011. We enrolled “discordant” couples where one partner was HIV infected, and the other was HIV negative. We were asking two questions: If we give antiviral treatment to HIV infected people earlier than usually started can we prevent HIV transmission to the negative sexual partner, and can we demonstrate that earlier treatment benefits the health of the person with infection?
“This was the ultimate public private partnership. The work we were doing was under IND (FDA-Investigational New Drug), but not seeking licensure approval for this purpose. The trial we conducted was called HPTN 052; the trial started around 2007, and addressed the primary endpoint of the hypothesis–prevention of HIV transmission–in 2011. We enrolled “discordant” couples where one partner was HIV infected, and the other was HIV negative. We were asking two questions: If we give antiviral treatment to HIV infected people earlier than usually started can we prevent HIV transmission to the negative sexual partner, and can we demonstrate that earlier treatment benefits the health of the person with infection?